
A continuing program of research and development is focusing on the use of controlled illumination by light-emitting diodes (LEDs) to treat mucositis and to accelerate healing of wounds. The basic idea is to illuminate the affected area of a patient with light of an intensity, duration, and wavelength (or combination of wavelengths) chosen to produce a therapeutic effect while generating only a minimal amount
of heat.
This method of treatment was originally intended for treating the mucositis that is a common complication of chemotherapy and radiation therapy for cancer. It is now also under consideration as a means to accelerate the healing of wounds and possibly also to treat exposure to chemical and radioactive warfare agents.
The present method offers an attractive alternative to hyperbaric-oxygen and laser treatments: It is not necessary to confine the patient to a hyperbaric chamber, treatment times are relatively short, LED arrays can illuminate large areas, and the exposure of the patient to heat generated by an LED array can readily be limited.
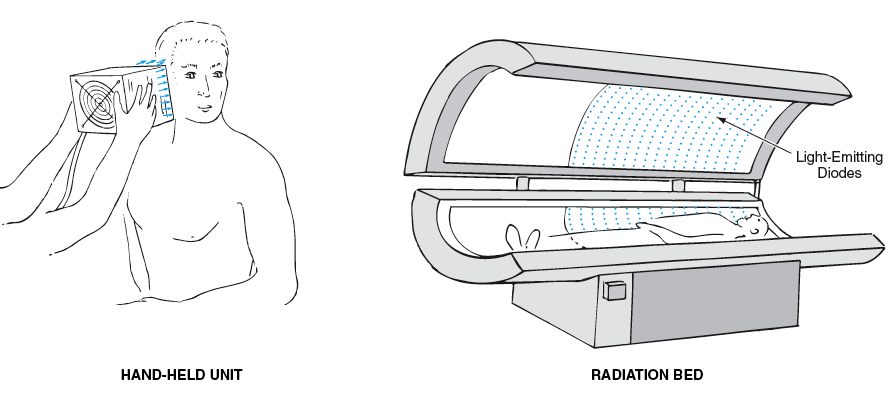
The figure depicts two examples representative of the range of sizes of treatment apparatuses according to the present method. The preferred sources of light in an apparatus of this type are substantially monochromatic doubleheterojunction GaAlAs LEDs arranged in an array large enough to expose the affected area of a patient uniformly at the required intensity. If light of a single wavelength is to be used, then the wavelength believed to be optimal for treating mucositis is 688 nm. If LEDs of 688-nm wavelength are not available, then one could use a three-wavelength combination (680, 730, and 880 nm) that is believed to be an optimal combination for treating mucositis; in this case, the LEDs of the three different wavelengths would be placed side by side in an array. Other single wavelengths and combinations of wavelengths may also be suitable.
In addition to the wavelength(s), the energy density should be chosen to maximize the biostimulatory effect. Moreover, the power density must exceed a threshold level in order to exert a biostimulatory effect. The optimal energy density has been determined to be about 4 J/cm2. This energy density could be delivered, for example, at a power density of 60 mW/cm2 (which exceeds the threshold) during an exposure time of 70 seconds. Such a short treatment time is particularly desirable for treating a young child.
This work was done by Robert W. Ignatius, Todd S. Martin, and Charles Kirk of Quantum Devices, Inc. for Marshall Space Flight Center.
In accordance with Public Law 96-517, the contractor has elected to retain title to this invention. Inquiries concerning rights for its commercial use should be addressed to: Ronald W. Ignatius, Founder & Chairman
Quantum Devices, Inc.
P.O. Box 100
112 Orbison Street
Barneveld, WI 53507
E-mail:
Refer to MFS-31651, volume and number of this NASA Tech Briefs issue, and the page number.